8 CRVS Champion: Dr. Amani SiyamOur community newsletter puts a spotlight on people who have gone above and beyond in their efforts to support CRVS programmes in Asia and the Pacific, raise awareness of CRVS issues or lead CRVS improvement efforts in their home country or in the region. This month, we would like to dedicate this issue of Insight to Dr. Amani Siyam What is your current title and role? I serve as the regional advisor for health information systems in the WHO Office for South-East Asia which supports eleven WHO member states home to over a quarter of the global population: Bangladesh, Bhutan, Democratic Peoples Republic of Korea, India, Indonesia, Maldives, Myanmar, Nepal, Sri Lanka, Thailand and Timor-Leste. Can you please share with us a particular experience which highlighted the importance of CRVS to you? I am particularly focused on ensuring populations are covered by basic health services and protection from a vicious cycle of financial hardship to access health care. These tenants of universal health coverage will be nowhere near met if every birth is not counted as a basic human right that unlocks the rights of access to descent services from health to education to civilian rights and if that opportunity is not equally availed to all segments of the population it becomes a chronic cause of all sorts of inequalities in accessing health and social care. In many countries of Asia and the Pacific, CRVS systems are short for substantial investments to improve their performance, and more drastic is how that suboptimal coverage impacts the lives and livelihoods of women and girls, coined as “the missing women phenomenon”, by Nobel laureate Amartya Sen. How are you currently involved in CRVS improvements? I have had the privilege to work in my own country’s bureau of national statistics where I gained exposure to the complexity of reporting mechanisms between where the vital events occur and how those are reported from the facility or community level to the local government and above. More complex to deal with is the linkage to the national identification system which remains somewhat ad hoc and opportunistic specially in low- and middle-income settings. I am currently involved with countries where the foundations of CRVS systems appear in place in terms of government regulations, legal frameworks and business processes mostly using paper-based systems that were established during colonial times. Faced with changing population dynamics, in terms of size, diversity and distribution, countries are left with clear gaps in attaining the mandatory coverage and completeness of vital registration and thus unable to make a strong investment case for public sector spending. Importantly, countries decision-makers are growingly becoming more aware of these implications, and we are witnessing different types of technical, financial and advocacy support being requested from WHO and CRVS-concerned global partners. Working with our partners, we aim to provide that support internal and external around a well-defined CRVS strategic action plan as the accountability framework of countries policy actions and investments. Which advice would you give to others trying to improve CRVS systems? I believe partnerships for CRVS is the best stroke to make a real and sustainable difference. Undoubtedly in every setting, the hierarchy of CRVS stakeholders is diverse in terms of needs, benefits, and interests (be it civil registrar officers, statisticians, demographers, researchers, law makers, local authorities, health facilities, health workers, communities, and the key beneficiaries the individuals themselves). Partnerships for CRVS must ensure that their contributions to countries CRVS system development are governed by a well-to-do CRVS strategic action plan or similar that is inclusive of all stakeholders, that clearly maps their functions, roles, responsibilities, and collective benefits, and that outlines strategic milestones to be achieved in terms of coverage, quality development and system maturity. Finally, countries experience with the COVID pandemic drastically exposed fundamental shortfalls in the recording and reporting of deaths and causes of death data. Partnerships for CRVS must give that aspect careful thinking and decide on how best to capitalize on the unequivocal digital health transformation unlocked by the pandemic response and beyond. Partnerships for CRVS can readily start by supporting countries to effectively implement ICD-11 suite of tools, in skilling up CRVS stakeholders in trusted data exchange and consequently in generating quality vital statistics that will can be readily available to all sorts of uses and users at the local, national and international levels. |

News & Events

15 Nov 2023
CRVS Champion: Dr. Amani Siyam

More News

25 November 2024
Newsletter Nov. 2024GHAI, Vital Strategies, ESCAP and other partners are supporting civil society…

25 November 2024
A new report by UNICEF Australia has revealed that thousands of Australian children are going…
25 November 2024
Newsletter Nov. 2024A new page on www.getinthepicture.org provides a list of CRVS related eLearning…

25 November 2024
Newsletter Nov. 2024The International Organization for Migration (IOM) has published its fourth…

25 November 2024
Newsletter Nov. 2024Sri Lankan President Anura Kumara Dissanayake has announced plans to implement…

25 November 2024
Newsletter Nov. 2024Papua New Guinea (PNG) is taking significant steps to reform its electoral…
25 November 2024
Newsletter Nov. 2024India's government has launched a new mobile app to simplify civil registration…

25 November 2024
ProvincesNewsletter Nov. 2024The National ID in Vanuatu is being introduced as the Hospital…

25 November 2024
Newsletter Nov. 2024Our community newsletter puts a spotlight on people who have gone above and…
25 November 2024
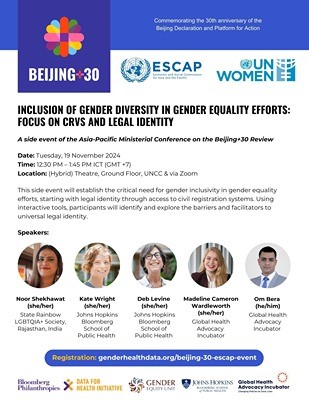
Newsletter Nov. 2024The Asia-Pacific Ministerial Conference on the Beijing+30 Review took place…